For your heavily treatment‑experienced patients with HIV whose current ARV regimen is failing and who need additional support to achieve long‑term suppression.1
Discover the Power of TROGARZO® observed in the TMB‑301 clinical trial:
TROGARZO®
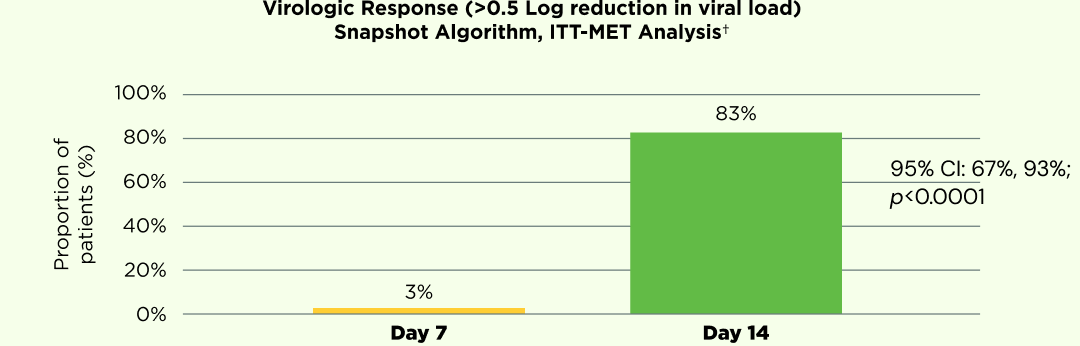
A powerful virologic response1
At 7 days post‑loading dose (Day 14 of the trial), 83% of patients who received TROGARZO® functional monotherapy achieved a virologic response vs. 3% of patients pre‑loading dose (p<0.0001; 95% CI: 67%, 93%).1
Data from the original TROGARZO® studies.
† A single‑arm, multicenter study of 40 heavily treatment‑experienced patients with multidrug resistant HIV‑1. Patients were required to have viral load >1000 copies/mL, documented resistance to at least 1 antiretroviral from at least 3 classes of antiretrovirals, been treated for at least 6 months and be failing or had recently failed therapy. Days 0‑6 (control period): Patients were monitored on their current failing regimens (or no therapy). Days 7‑13 (functional monotherapy period): Patients continued on background failing regimens and received 2000 mg of TROGARZO® (loading dose). Day 14: Background regimen was optimized to include at least one active agent. Day 21‑Week 25 (maintenance period): Patients received 800 mg of TROGARZO® every 2 weeks (maintenance dose). The primary efficacy endpoint was the proportion of patients achieving a -0.5 log10 decrease in viral load during the functional monotherapy period compared with the proportion of patients achieving a -0.5 log10 decrease during the control period.1
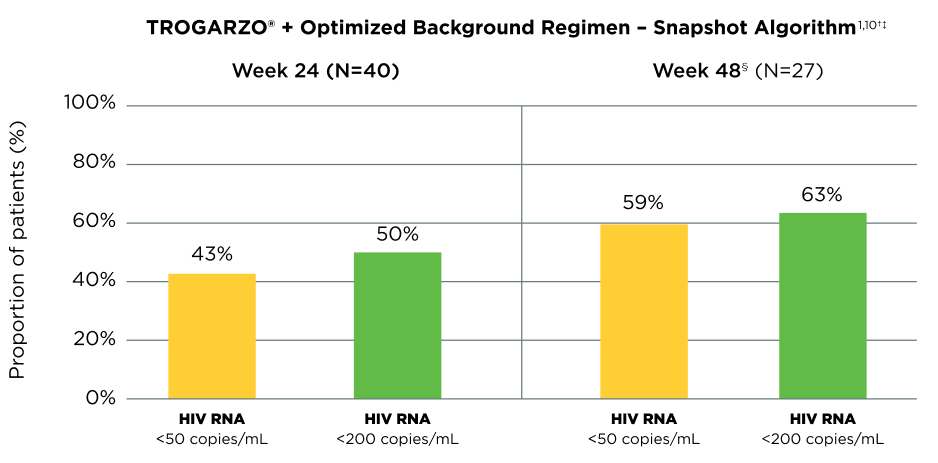
Providing durable viral suppression1,10
Data from the original TROGARZO® studies
Patients who achieved HIV RNA <50 copies/mL at Week 24 maintained viral suppression up to Week 4810§
† A single‑arm, multicenter study of 40 heavily treatment‑experienced patients with multidrug resistant HIV‑1. Patients were required to have viral load >1000 copies/mL, documented resistance to at least 1 antiretroviral from at least 3 classes of antiretrovirals, been treated for at least 6 months and be failing or had recently failed therapy. Days 0‑6 (control period): Patients were monitored on their current failing regimens (or no therapy). Days 7‑13 (functional monotherapy period): Patients continued on background failing regimens and received 2000 mg of TROGARZO® (loading dose). Day 14: Background regimen was optimized to include at least one active agent. Day 21‑Week 25 (maintenance period): Patients received 800 mg of TROGARZO® every 2 weeks (maintenance dose). The primary efficacy endpoint was the proportion of patients achieving a -0.5 log10 decrease in viral load during the functional monotherapy period compared with the proportion of patients achieving a -0.5 log10 decrease during the control period. ‡ TROGARZO® + Optimized Background Regimen – snapshot algorithm. Undetectable viral load is defined as fewer than 50 copies per mL of blood.1 § 48‑week data is not included in the TROGARZO® prescribing information.
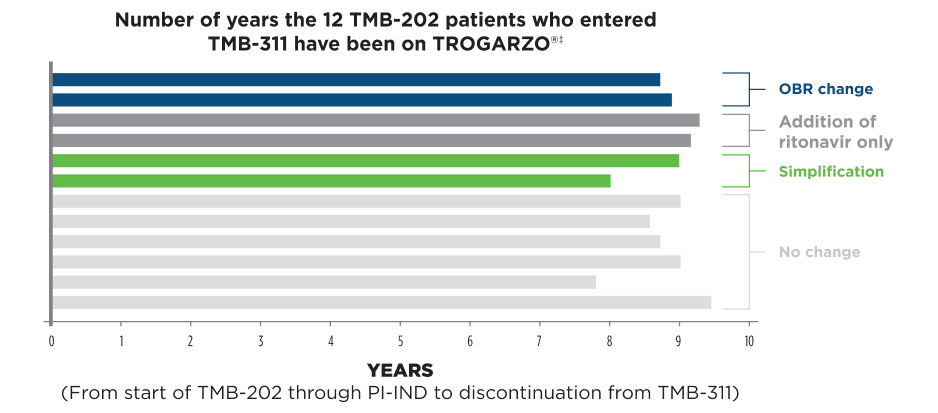
Long-term data from a subset of TMB‑202 (Phase 2b) patients11†
Outcomes11
Number of total TROGARZO® infusions ranged from approximately 203 to 247
Durability of response maintained with minimal adjustments to OBRs
6 patients had no changes to their OBRs
2 patients had one medication removed from their OBR
4 patients had a change to their OBR
† These results were not included in the Biologics License Application (BLA), and were therefore not reviewed by the FDA to support the approval of TROGARZO®. These patients were enrolled in a Phase 2b study (TMB‑202). At the end of the study, patients continued to receive TROGARZO® under an investigator‑sponsored Investigational New Drug (PI‑IND) until they entered the TMB‑311 expanded‑access protocol. Durability data include the total time on therapy in TMB‑202, PI‑IND, and TMB‑311. ‡ Study investigators chose to continue or discontinue patients after TMB‑202 with no further support other than ibalizumab study drug.11
TROGARZO® is for HTE patients with HIV whose current ARV regimen is failing and who need additional support to achieve long‑term suppression.1
TROGARZO® Clinical Trial: TMB‑301
Description
Trial TMB‑301 was a single‑arm, multicenter clinical trial that evaluated the efficacy and safety of TROGARZO® in heavily treatment‑experienced patients who have multidrug resistant HIV‑1.1
Participants were considered for inclusion if they had:1
A baseline viral load >1,000 copies/mL, and
Documented resistance to ≥1 ARV from each of 3 classes of ARV medications as measured by resistance testing
Prior treatment with ARVs for ≥6 months but whose therapy was failing or had recently failed (i.e., in the 8 weeks prior to enrollment)
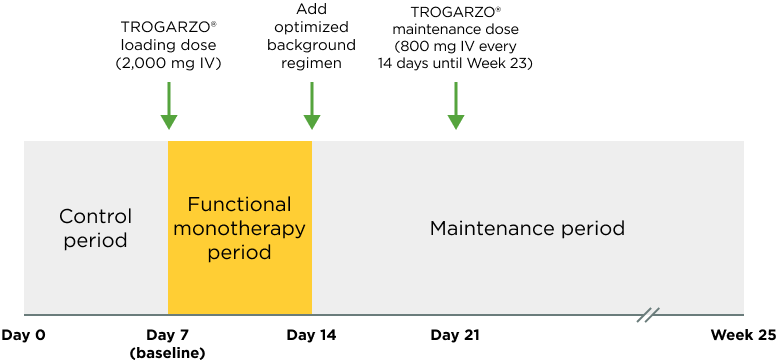
Trial Design1,12
Trial TMB‑301 was composed of 3 discrete periods:12
Control Period1(Day 0 to Day 6)
Participants were either monitored on their current failing therapy or received no therapy if they had failed and discontinued treatment within 8 weeks prior to screening.1
This was an observational period to establish baseline HIV‑1 viral load
Functional Monotherapy Period1(Day 7 to Day 13)
All participants received a 2,000 mg loading dose of TROGARZO® on Day 7. Those on a failing ARV regimen continued to receive their failing regimen in addition to the loading dose of TROGARZO®.1
This period was to establish the virologic activity of TROGARZO®
Maintenance Period1(Day 14 to Week 25)
On Day 14, viral load was assessed for the primary endpoint, and thereafter the background regimen was optimized to include at least 1 drug to which the participant’s virus was susceptible. The use of investigational drug(s) as a component of this regimen was allowed.1
Beginning at Day 21, an 800 mg maintenance dose of TROGARZO® was administered through Week 25.1
This period was to establish the safety and durability of virologic suppression of TROGARZO® when used in combination with an optimized background regimen
Important Safety Information
Indication
TROGARZO® (ibalizumab‑uiyk), in combination with other antiretroviral(s), is indicated for the treatment of human immunodeficiency virus type 1 (HIV‑1) infection in heavily treatment‑experienced adults with multidrug resistant HIV‑1 infection failing their current antiretroviral regimen.
Contraindications
TROGARZO® is contraindicated in patients with a prior hypersensitivity reaction to TROGARZO® or any components of the product.
Use in Specific Populations
Pregnancy: No adequate human data are available to establish whether or not TROGARZO® poses a risk to pregnancy outcomes. Monoclonal antibodies, such as ibalizumab‑uiyk, are transported across the placenta as pregnancy progresses; therefore, ibalizumab‑uiyk has the potential to be transmitted from the mother to the developing fetus.
Lactation: No data are available regarding the presence of TROGARZO® in human milk, the effects on the breastfed child, or the effects on milk production. Because of the potential for HIV‑1 transmission, instruct mothers not to breastfeed if they are receiving TROGARZO®.
Warnings and Precautions
Hypersensitivity Including Infusion‑Related and Anaphylactic Reactions
Hypersensitivity reactions including infusion‑related reactions and anaphylactic reactions have been reported following infusion of TROGARZO® during post‑approval use. Symptoms may include dyspnea, angioedema, wheezing, chest pain, chest tightness, cough, hot flush, nausea, and vomiting. If signs and symptoms of an anaphylactic or other clinically significant hypersensitivity reaction occur, immediately discontinue administration of TROGARZO® and initiate appropriate treatment. The use of TROGARZO® is contraindicated in patients with known hypersensitivity with TROGARZO®.
Immune Reconstitution Inflammatory Syndrome
Immune Reconstitution Inflammatory Syndrome (IRIS) has been reported in one patient treated with TROGARZO® in combination with other antiretrovirals. During the initial phase of combination antiretroviral therapies, patients whose immune systems respond may develop an inflammatory response to indolent or residual opportunistic infections, which may necessitate further evaluation and treatment.
Embryo-Fetal Toxicity
Based on animal data, TROGARZO® may cause reversible immunosuppression (CD4+ T cell and B cell lymphocytopenia) in infants born to mothers exposed to TROGARZO® during pregnancy. Immune phenotyping of the peripheral blood and expert consultation are recommended to provide guidance regarding monitoring and management of exposed infants based on the degree of immunosuppression observed. The safety of administering live or live‑attenuated vaccines in exposed infants is unknown.
Adverse Reactions
The most common adverse reactions (all Grades) seen in clinical trial experience, reported in at least 5% of subjects receiving TROGARZO® were diarrhea (8%), dizziness (8%), nausea (5%) and rash (5%).
Most (90%) of the adverse reactions reported were mild or moderate in severity. Two subjects experienced severe adverse reactions: one subject had a severe rash and one subject developed IRIS manifested as an exacerbation of progressive multifocal leukoencephalopathy.
To report suspected adverse reactions, contact THERA patient support® at 1‑833‑23THERA (1‑833‑238-4372) or FDA at 1‑800‑FDA-1088 or www.fda.gov/medwatch.